If you’ve ever typed “help for depression” into a search bar at 2 a.m., you already know the internet loves to drown you in options without actually helping you choose. CBT, DBT, EMDR, talk therapy, psychodynamic, the list goes on, and nobody tells you which one is right for you.
Here’s the honest truth: there’s no single “best” therapy for depression. But there are therapies that work far better for specific situations, personalities, and severities of depression. Understanding the difference could save you months of spinning your wheels with the wrong approach.
This guide breaks it all down, plainly, practically, and without the clinical jargon that makes most mental health content feel like a textbook.
Before comparing types of therapy for depression, it helps to understand what therapy is trying to do. Depression isn’t just sadness, it’s a disruption in how you think, feel, and behave. Effective therapy targets at least one of those three layers.
Some approaches work top-down (changing thoughts to shift emotions). Others work bottom-up (using the body and nervous system). Some go deep into your past; others focus entirely on your present behavior. The “best” one depends on where your depression is rooted.
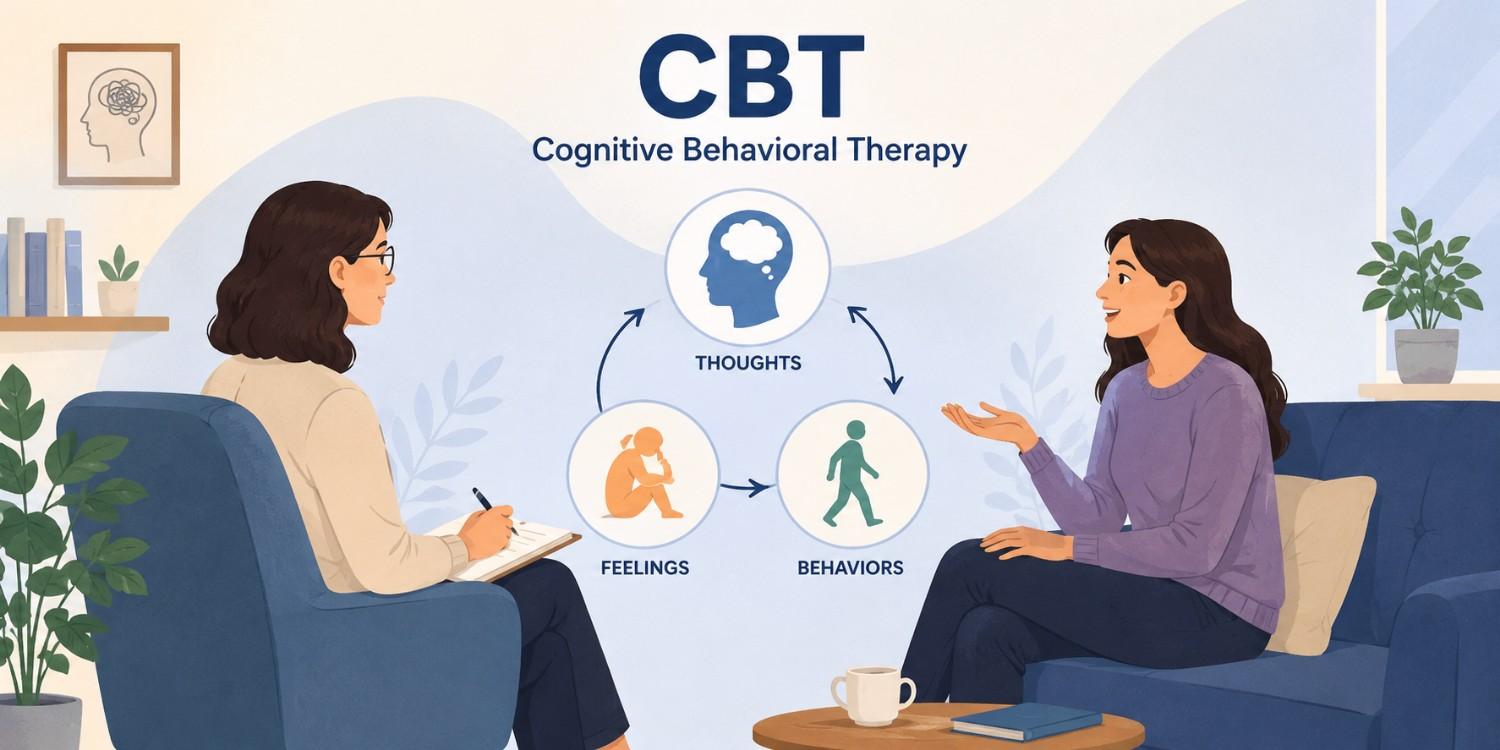
CBT is probably the most researched and widely recommended therapy for depression in the world and for good reason. It’s structured, goal-oriented, and typically runs 12 to 20 sessions.
The core idea: your thoughts drive your emotions. When you’re depressed, your thinking patterns tend to be distorted, you catastrophize, overgeneralize, or assume the worst. CBT helps you identify those patterns, challenge them, and replace them with more balanced thinking.
Research consistently backs CBT. A landmark review published in Cognitive Therapy and Research found that CBT was as effective as antidepressant medication for moderate depression and significantly reduced relapse rates compared to medication alone.
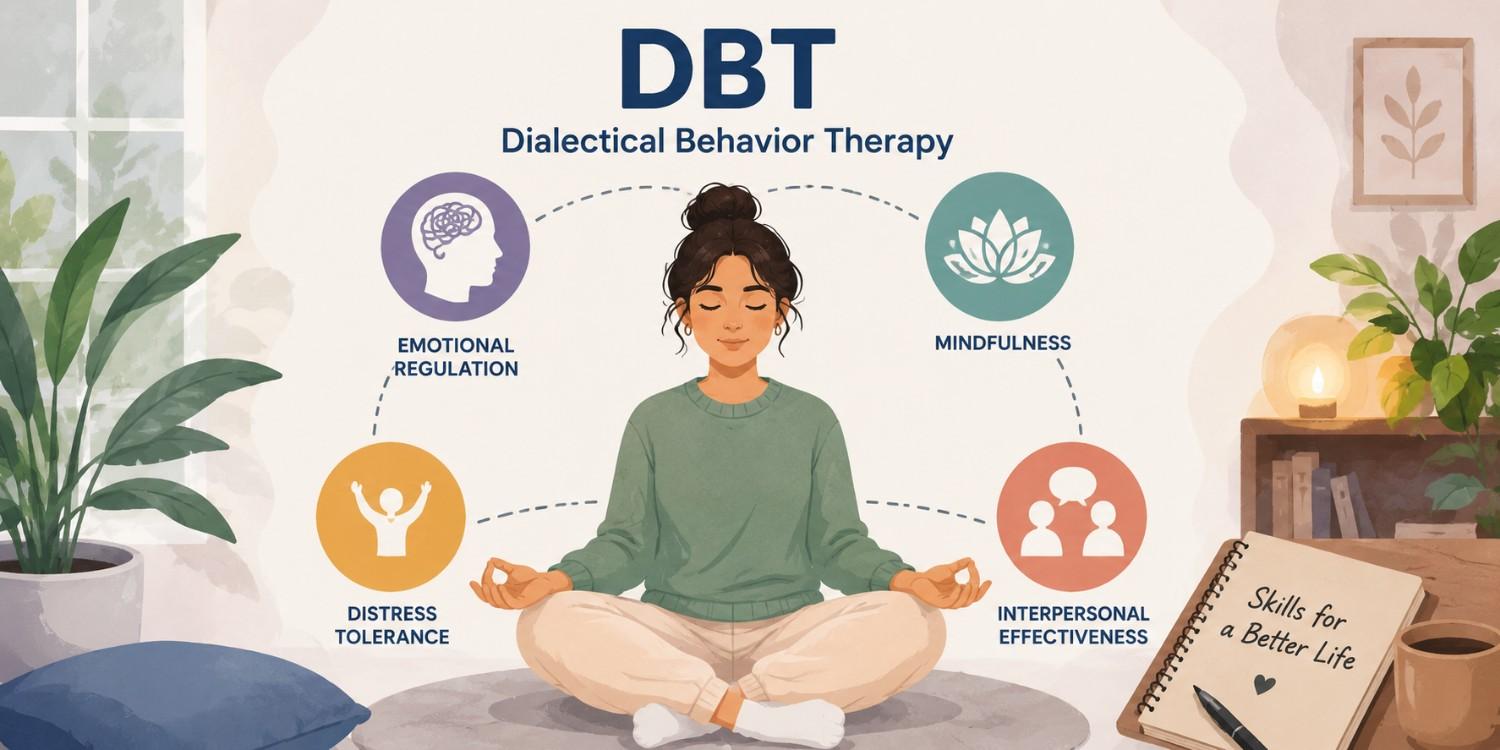
Originally developed for borderline personality disorder, DBT has become a go-to for people whose depression comes with intense emotional swings, self-harm urges, or difficulty managing relationships.
DBT blends cognitive-behavioral techniques with mindfulness-based strategies. It teaches four core skill sets: emotional regulation, distress tolerance, interpersonal effectiveness, and mindfulness.
If CBT is a scalpel, DBT is more of a full-body toolkit.

This is the therapy that actually explores your past, your childhood, your attachment patterns, your unconscious beliefs. It’s less structured than CBT and often runs longer (months to years in some cases).
Psychodynamic therapy is rooted in the idea that unresolved emotional conflicts, often stemming from early relationships, manifest as depression in adulthood. By bringing those patterns to light, you can begin to untangle them.
A 2017 study in JAMA Psychiatry found that psychodynamic therapy produced lasting symptom improvement even after treatment ended a phenomenon researchers called the “sleeper effect.”

IPT is laser-focused on one thing: your relationships. It operates on the premise that depression often emerges from, or is worsened by, problems in your interpersonal world, grief, role transitions, conflict, or social isolation.
Typically brief (12 to 16 sessions), IPT helps you identify which relationship pattern is fueling your depression and gives you concrete skills to address it.
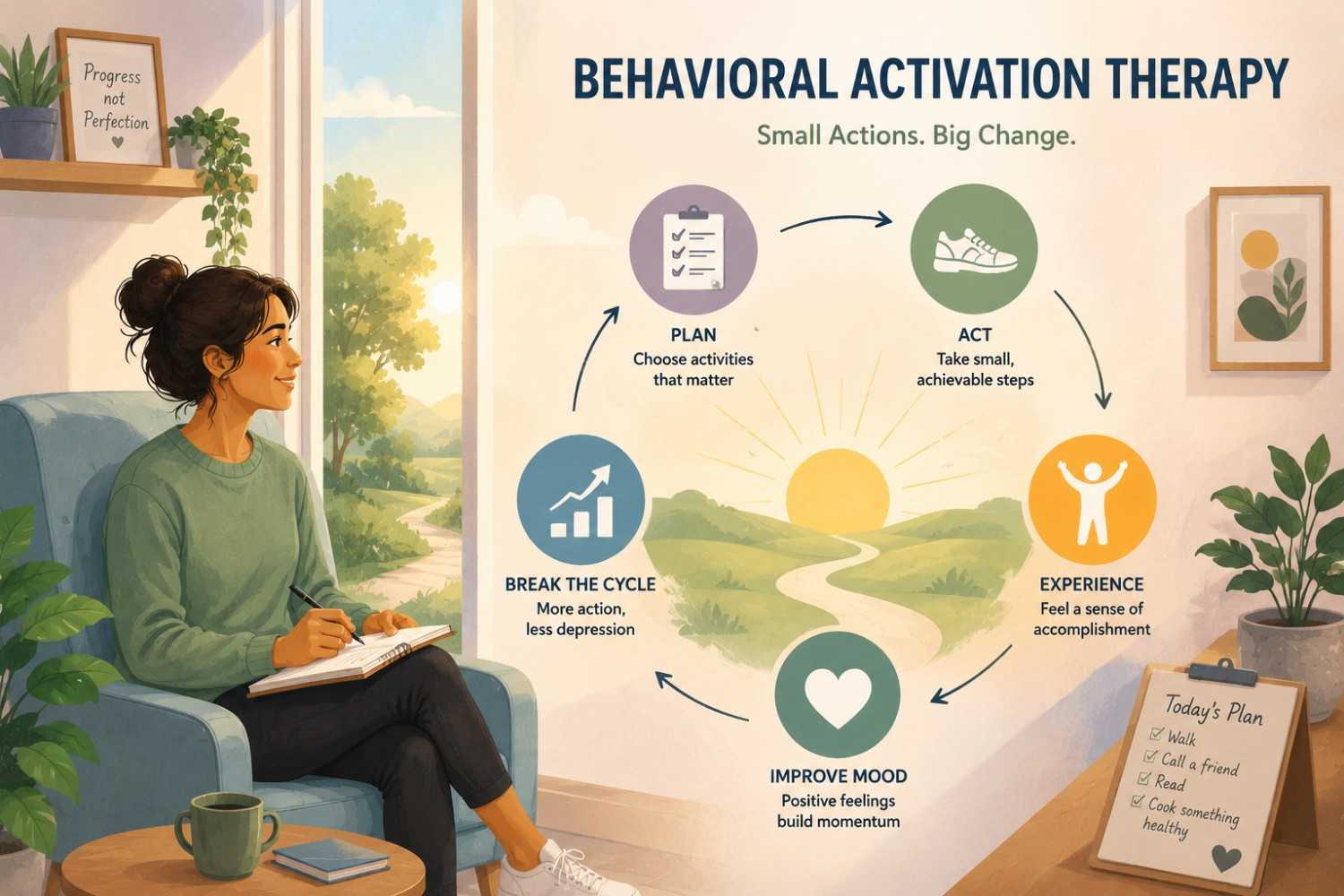
One of the most underrated types of therapy for depression, behavioral activation is deceptively simple: depression makes you withdraw, and withdrawal makes depression worse. The goal is to break that cycle by gradually re-engaging with rewarding activities.
It doesn’t require deep introspection. You don’t have to relive trauma. You just start doing things small, intentional things, that give your brain a reason to re-engage with life.

EMDR was originally developed for PTSD, but therapists increasingly use it for depression, particularly when depression is rooted in past trauma or adverse experiences.
It uses bilateral stimulation (usually guided eye movements) to help the brain process distressing memories that haven’t been fully integrated. It sounds unusual, but the evidence base is growing steadily.
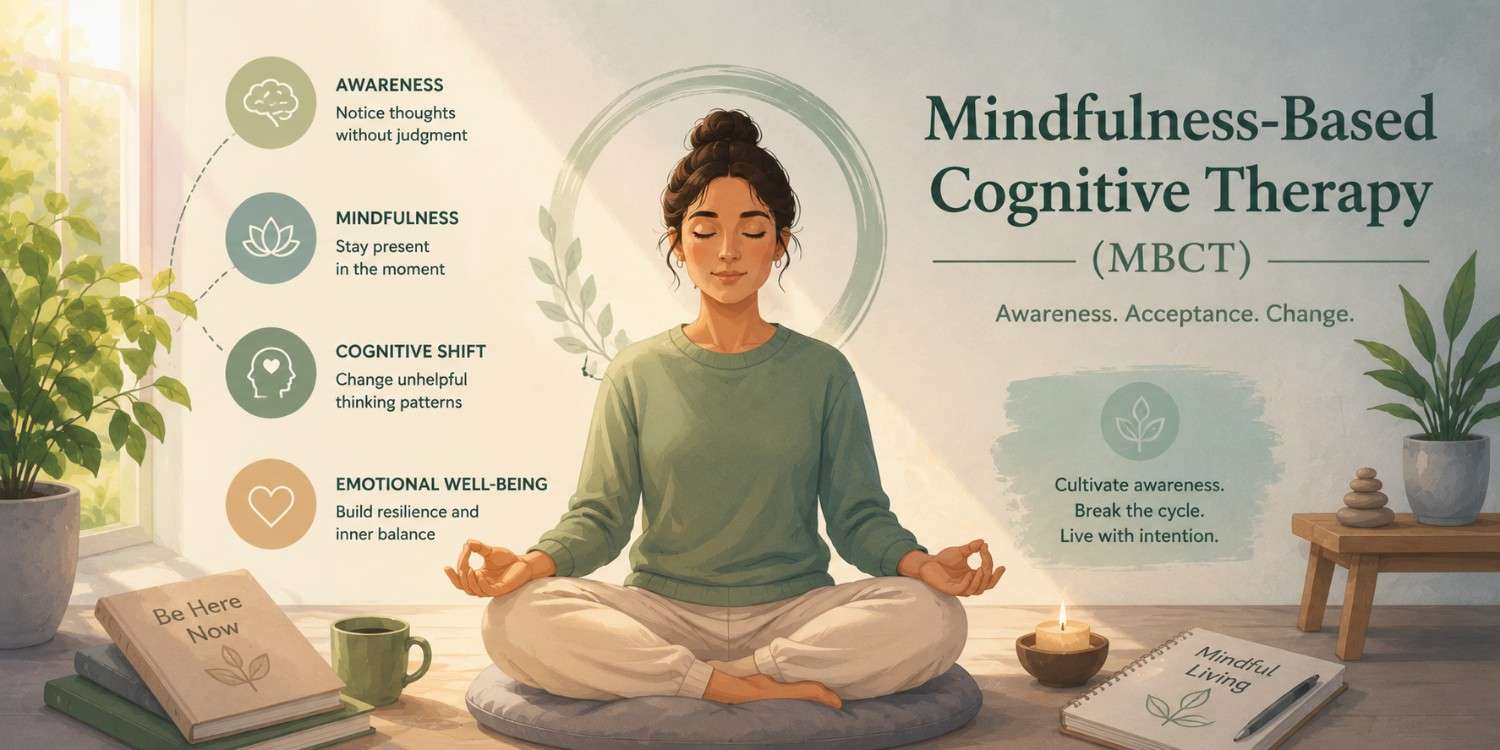
MBCT is specifically designed to prevent depression relapse. It combines mindfulness meditation practices with CBT techniques to help people recognize early warning signs of a depressive episode and respond differently.
Studies show MBCT reduces relapse rates by up to 43% in people with three or more previous depressive episodes, making it one of the most powerful long-term tools available.
The research points to CBT as the most broadly effective starting point, it works across age groups, depression severities, and delivery formats (in-person, online, even app-based). But “best overall” doesn’t mean “best for you.”
Here’s a quick framework:
And sometimes, the most effective approach is a combination, therapy alongside medication, or integrating elements of CBT with mindfulness practices. A good therapist will help you figure this out rather than rigidly sticking to one modality.
Navigating depression is hard enough without also having to decode the therapy landscape on your own. The good news? You don’t have to get it perfect on the first try. Most people find their way to the right fit through a little trial and reflection and that’s completely normal.
What matters most is starting. Whether that’s CBT, DBT, or a conversation with your GP about where to begin, the act of reaching out is itself a meaningful step. Depression lies to you and tells you nothing will help. The evidence says otherwise.
Cognitive Behavioral Therapy (CBT) is the most widely researched and recommended therapy for depression. It has strong evidence for mild to moderate depression and is available in many formats, including online. That said, effectiveness depends on the individual, other approaches like psychodynamic therapy or MBCT may work better for chronic or recurring depression.
Most people begin to notice improvement after 6 to 8 sessions, though this varies by therapy type and severity. CBT is typically structured over 12 to 20 sessions. Psychodynamic therapy and other open-ended approaches may continue for months or years depending on the goals.
Yes, for mild to moderate depression, therapy alone, particularly CBT can be as effective as antidepressant medication. For severe depression, a combination of therapy and medication tends to produce the best outcomes. This is something to discuss with a mental health professional based on your specific situation.
For depression that hasn’t responded to standard treatments, options include psychodynamic therapy, EMDR (especially if trauma is a factor), and newer approaches like ketamine-assisted therapy or transcranial magnetic stimulation (TMS) in combination with psychotherapy. A psychiatrist can help evaluate these options.
Research suggests that online CBT is nearly as effective as in-person CBT for mild to moderate depression. Platforms offering live video sessions with licensed therapists tend to produce better outcomes than purely self-guided apps. For severe depression or complex presentations, in-person therapy is generally recommended.
CBT focuses on identifying and changing distorted thought patterns that contribute to depression. DBT expands on this by adding skills for emotional regulation, distress tolerance, and mindfulness, making it particularly useful when depression involves intense emotional swings or self-destructive behaviors. Both are evidence-based and effective; the right choice depends on your specific symptoms and patterns.
National Institute of Mental Health (NIMH) — Depression Treatment Overview The NIMH, America’s leading federal mental health research authority, confirms that CBT and Interpersonal Therapy are among the most evidence-backed treatments for depression. This page covers psychotherapy, medication, and brain stimulation options in a comprehensive, clinically grounded overview.
American Psychological Association (APA) — Depression Treatments for Adults The APA’s official clinical guideline page breaks down CBT, psychodynamic therapy, and Interpersonal Therapy in detail, including when each is recommended and why. It’s one of the most authoritative sources for understanding how therapy choices are made in real clinical settings.
PubMed/NIH — CBT vs. Digital CBT: A Systematic Review (2022) This peer-reviewed systematic review analyzed 106 studies covering 11,854 patients. It found that both face-to-face and digital CBT are effective for depression, with human-guided digital formats producing results closest to in-person therapy, directly supporting the blog’s point on online therapy effectiveness.
Pearlman & Associates is a trusted St. Louis-based therapy practice known for delivering high-quality, evidence-based mental health care. Our team of licensed and experienced therapists works with children, teens, adults, couples, and families, helping them navigate anxiety, depression, stress, trauma, and relationship challenges. We combine clinical expertise with a personalised approach to ensure every client receives care tailored to their unique needs. With a strong focus on confidentiality, ethical practice, and long-term results, we create a safe, supportive environment where real progress happens. To connect with our team, call 314-942-1147 or email bryan@stlmentalhealth.com